



Ever wondered what are some other differences between these preparations, besides appearance, texture, and feel?
In addition to the previously mentioned. There are also pastes, foams, and jellies. All these topical treatments are types of vehicles, that usually carry the drug -the active ingredient(s)-. They could also be unmedicated, to serve as lubricants or protectants of the skin. The drug -the active ingredient(s)– is either, dissolved in the vehicle, or undissolved (suspended).
They are designed to be semi-solid in nature allowing them to form a film when applied onto the skin.
These vehicles are designed to stay in contact with the skin for a reasonable amount of time (facilitating drug absorption through the skin, into the affected area, or systemically to the body) before they are removed or washed off intentionally or unintentionally. In other words, when you allow the preparation to sit on your skin for a reasonable amount of time, you are allowing the medication in these vehicles the maximum time to be absorbed into your skin. The vehicle itself, however, might evaporate from the skin, but not completely, because other oily parts stay on the skin until you physically remove them.
These topical preparations are designed to either;
- Give local dermal effects to the area treated, i.e. like most dermatological products to treat skin problems.
Or
- Give systemic transdermal effects through the skin, into the underlying tissue, or to the systemic blood circulation going to other tissues of the body. An example is hormonal therapy through gel application on the skin.
Note: Drugs that are toxic in small concentrations, can not be prepared in topical preparations, because the dose of application is not accurate. When we counsel patients, we either say, use liberally, or use sparingly, for example, there is no fixed measurement usually, and even if there was, the exact amount of drug absorbed through the skin can only be measured predictably but not accurately.
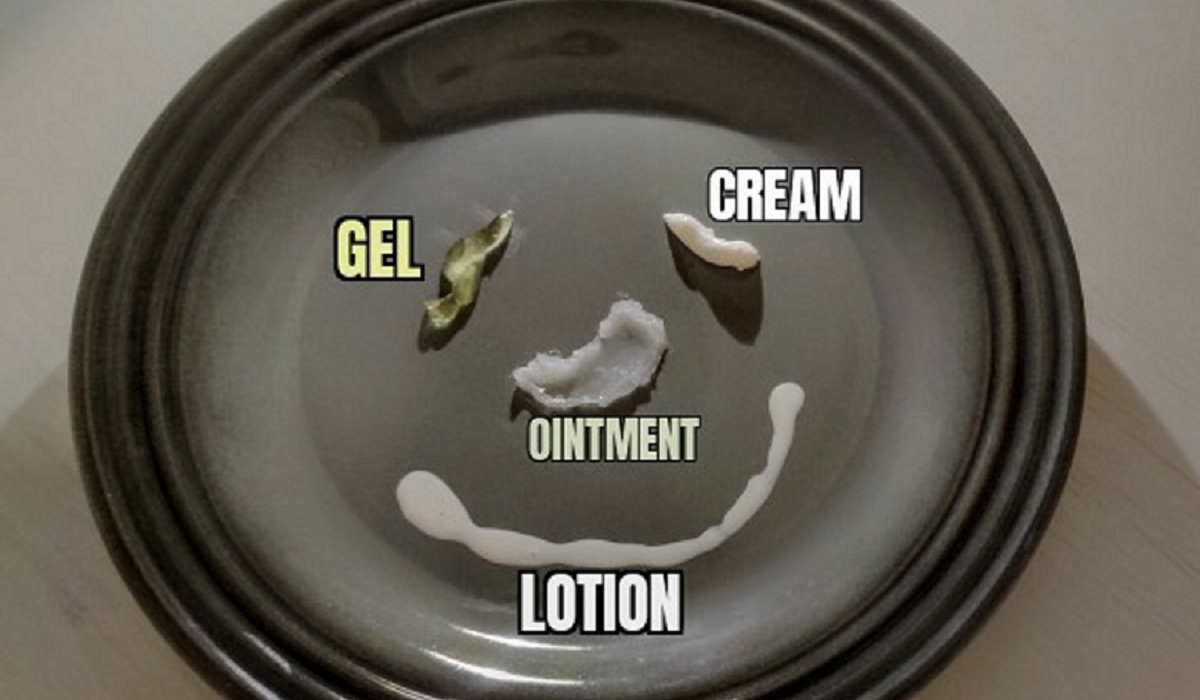
Now, what are the differences between different types of topical preparations?
Ointments
- More than 50% oil/lipid based
- Water less than 20%
- Semi-solids that often soften or melt at body temperature
- Spreads smoothly and easily and have non gritty feel, but could be greasy
- Applied externally on the skin, or inside openings of the body from the skin, like inner mouth cheeks, or the vagina
- Typically used as; emollients (locking in moisture, hydrating), protective barriers (forming an occlusive film), and also serve as vehicles for some drugs -that dissolve in lipid- Example, Steroids
- They are preferred for their lubricating and occlusive properties, especially for dry or severe skin conditions, and also for thicker areas of the skin, where they lubricate, protect, and allow the medication within, a longer time to be absorbed into the skin
- Not preferred sometimes because they are cosmetically unappealing, for their annoying greasy, sticky feel, or simply to avoid causing other complications, like folliculitis (because of their occlusive film)
- No preservatives or other surfactant emulsifiers, or other agents, are usually needed, therefore they are not necessarily irritating to the skin
Creams
- Types of ointment with larger percentage of water than regular ointments
- Some are more oily, others are less oily depending on the ratios of water and oil in the cream preparation, but they are generally less oily than ointments
- More cosmetically acceptable
- Preferred over ointments as medicated vehicles, but they require special techniques in preparation
- Used for medicating, cleansing, and softening of the skin depending on their oil/water percentages
- A cream with more water than oil in it, if medicated, the drug is dissolved in the water part, but once the cream is applied to the skin, the water evaporates leaving the drug better suited in the oil film, enhancing its absorption through the skin
- A cream with more oil than water is usually used for cooling, softening, and cleansing of the skin. The cooling effect comes from the slower evaporation of its water content over time. The softening effect comes from its oil content that locks in moisture. They are generally gentler cleansers than water-based ones because they do not strip away natural oils of the skin
- Creams could be sensitizing because they might contain preservatives, detergents, scents, and emulsifier agents
Lotions
- They are like creams in every aspect generally, but they are more runny, less viscous formulations because they have a higher water content
- Their advantages over creams come in handy in hairy areas, like the head scalp, in oily skin prone to acne or simply because they are nongreasy and are sometimes more cosmetically appealing
- Another advantage is that a small amount of lotion can spread more easily and widely over the skin, and generally cost less, economically
- They are used as delivery vehicles for medications, like medicated shampoos and scalp lotions, for soothing and protection, like Calamine lotion. And also used for cosmetics or other aids
- Once again because of their aqueous content, they may contain preservatives, detergents, and emulsifiers that could be skin sensitizing
Gels
- Gels are topical formulations that include medications dissolved in water or other (hydrophobic) solvents and thickened with a gelling agent to form a polymer.
- They contain no oil
- Form a more stable film -than lotions, creams, and ointments- on the skin and allow the medication longer contact for absorption
- Provide a cooling sensation because the solvent part evaporates when the gel is applied on the skin, however, it might leave the skin dry afterwords
- Contain preservatives and other additives that could be irritating to the skin
- Gels and jellies have generally the same principle formulation, which is a drug in an aqua phase that is gelled or thickened with an agent. However, gels use gelling agents, to form polymers with a solvent (water or hydrophobic), jellies use thickening agents but usually only with water solutions. Gels are usually the advanced formulation used in medicated topicals.
What about pastes and foams?
My bonus 🙂
Since you’ve made it until here, then here is your bonus 😉
Pastes
- The amount of solids in pastes is high, therefore they have thicker, stiffer, and sometimes have a more gritty feel to them
- Their base could be either lipid based or aqueous gel based. They carry one or more medications in them
- Pastes are well adsorbed (retained) on the skin, and easily water washable (advantage when applied on traumatized skin)
- Pastes may well absorb water, therefore they are useful for oozing skin lesions
- Toothpastes are medicated with fluoride salts, the solid part of the paste provides an abrasive (scrubbing) effect for cleansing purposes. Zinc oxide paste is another example.
Fun Facts 🙂
Foams
- Are pressurized solutions with ethanol (as a propellant). When we aerosolize the solution into the air, the ethanol evaporates leading to the expansion of the medicated liquid droplets, which entrap air, and form the foam 🙂
- Foams are sometimes used because they are less irritating, example; acne skin, or for hard to reach areas of the skin like hairy scalp.
Creams have a whitish, creamy appearance, which is a result of scattering of light from their dispersed phases, such as oil globules. This distinguishes them from simple ointments, which are translucent.
Gels have an interesting physical -behavioural- phenomenon, depending on the force and speed applied, and their specific composition. Their gel form changes either;
- Becomes more liquid when you shake it
- Becomes a thicker gel when you shake it
- Continues to thin out when you fix the force and the speed of shaking
Isn’t that cool? 🙂
References, Citations, and Attributions:
Ram I. Mahato. Ajit S. Narang. Pharmaceutical Dosage Forms and Drug Delivery. CRC Press; Taylor & Francis Group. 2018
Zsikó, S.; Csányi, E.; Kovács, A.; Budai-Szűcs, M.; Gácsi, A.; Berkó, S. Methods to Evaluate Skin Penetration In Vitro. Sci. Pharm. 2019, 87, 19.


